For the year and a half, we’ve been extremely lucky to be able to provide bi-annual professional development for our dental technicians and clinic assistants. It has quickly become one of my favorite parts of our project. Jevaia dental clinics deliver the Basic Package of Oral Care, a collection of dental procedures that was designed in collaboration with the World Health Organization for limited-resources settings. The BPOC was developed by Europeans, and it has mostly been used in developing world settings as aid or transient care.
For the year and a half, we’ve been extremely lucky to be able to provide bi-annual professional development for our dental technicians and clinic assistants. It has quickly become one of my favorite parts of our project. Jevaia dental clinics deliver the Basic Package of Oral Care, a collection of dental procedures that was designed in collaboration with the World Health Organization for limited-resources settings. The BPOC was developed by Europeans, and it has mostly been used in developing world settings as aid or transient care.
Since we train local dental technicians to provide the BPOC in Health Posts instead of temporary camps or outreach programs, we’ve had the chance think about applying it as a sustained primary health care strategy–especially since we started working with Berkeley, Dr. Bethy and Dr. Keri and other collaborators in 2016. I suppose that kind of thinking is one difference between aid, or any kind of temporary relief, and human rights, which entitles people to a consistent standard of health care.
 Our past three professional development workshops have focused on the use of Silver Diamine Fluoride; infection control tailored to rural Health Posts; and treatment planning (one thing about a stable primary care provider is: they can actually plan!). This summer, Dr. Bethy is teaching our professional development on school-based treatment planning, so we can shift to a more systematic school-based oral health care model with local dental technicians.
Our past three professional development workshops have focused on the use of Silver Diamine Fluoride; infection control tailored to rural Health Posts; and treatment planning (one thing about a stable primary care provider is: they can actually plan!). This summer, Dr. Bethy is teaching our professional development on school-based treatment planning, so we can shift to a more systematic school-based oral health care model with local dental technicians.
Dental technicians in JOHC already conduct monthly school seminars to do school-based screening and treatment for children and parents. We call these “seminars” rather than “camps” because they are run by a local provider and they help connect people with the Health Post dental clinic. Unlike most “camps,” seminars don’t aim to treat as many teeth as possible in the shortest time, but to build relationships with the technician and raise public support for a government dental clinic and community outreach programs.
Our 2018 summer professional development was seven days long for veteran technicians and ten days for new technicians. It kicked of with technicians and assistants examining photos of real ART fillings (like the kind they do) organizing them in to acceptable and unacceptable outcomes. Then the clinicians had to use the photos to diagnose why the unacceptable treatments had partly or fully failed, which lead to a review of practice technique. It was really gratifying to see how this impacted everyone’s thinking a few days later, when we were back in a school placing fillings.
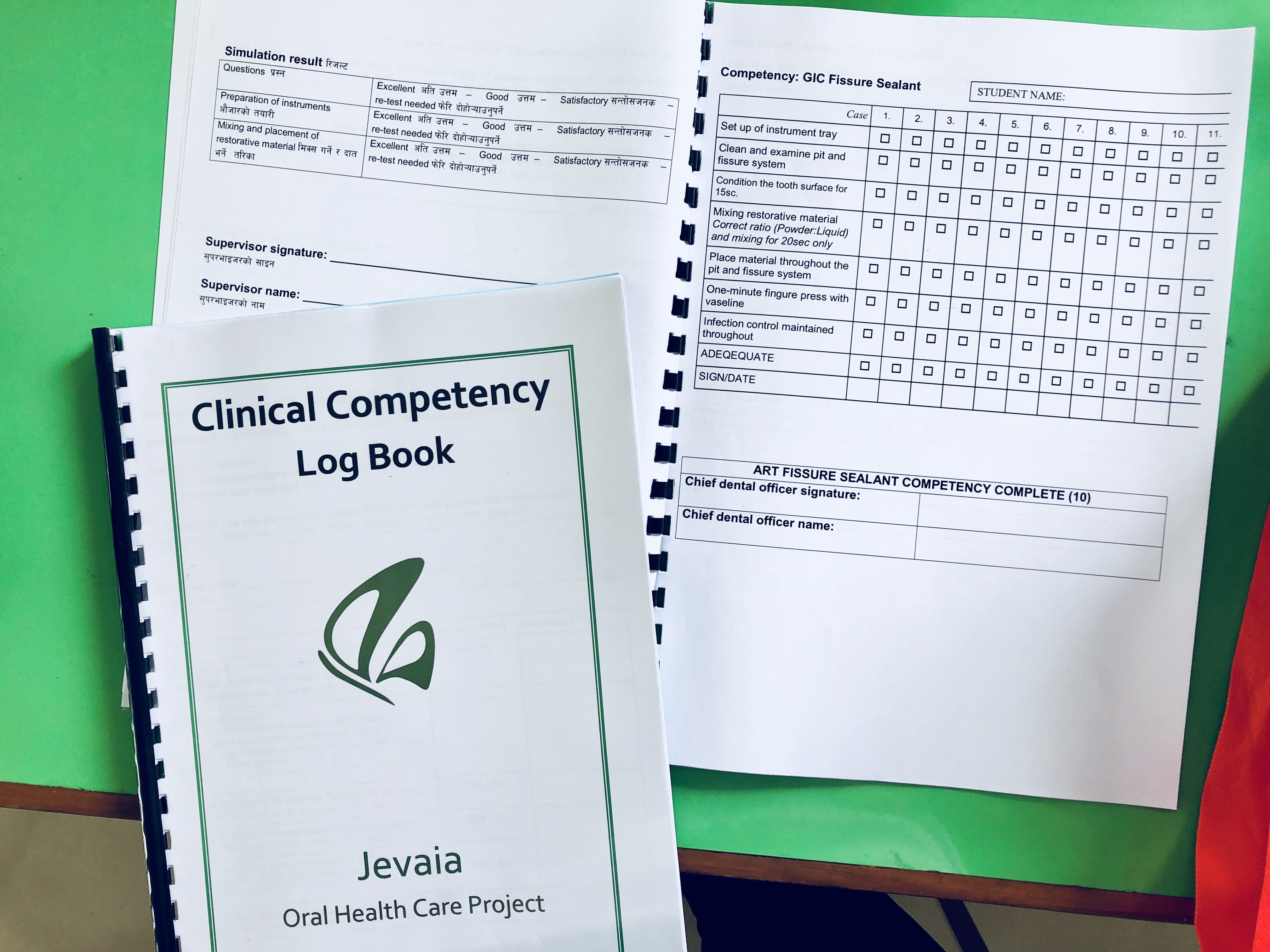
Since the BPOC was originally conceptualized as crisis management, a challenge of our project establishing a quality of care standard in a stable primary care setting. At this year’s workshop Bethy helped introduce a competency framework. During the three days of classroom work, our new technicians supervised old technicians in a “simulation seminar” where they had to demonstrate each technique using the competency checklist. When we moved to the three-day school setting with live patients, new technicians were supervised through ten of each procedure and had to pass the competency checklist ten times. Veteran technicians performed one of each technique under a doctor’s supervision and we used the completed checklists to award “competency certifications” that are valid for 18 months. We even created a framework for technicians to review their competency certification every 1-2 years.

Overall, the workshop was meant to guide our clinical teams toward a more rigorously informed, holistic approach to school-based health care, where JOHC technicians work as members of the primary care system rather than visitors. The training emphasized taking time to slow down and connect with patients rather than blowing through a line at the door. Dentistry can be scary and rather than jumping straight at a kid’s teeth, the intake leaves time to comfort frightened children and to learn about their lifestyle habits and disease risk factors. In turn that information is used to provide more complete and well-informed care, instead of just treating as many teeth as possible. It seems obvious, especially for primary care practice, but in reality that’s not usually how dentistry is done in our setting (or often, in general, if we’re being honest). As part of this, the clinical teams spent a good amount of time reviewing cariology (the biology of oral disease) which unlike the practicalities of how to mix cement and apply it properly, informs which techniques should be used when. In other words, without adding in more high-technology interventions, we are focusing on more effective deployment of the conventional BPOC.

For me as a non-clinician, it’s super interesting to see how these minimally-invasive techniques can be used not only for emergency management of foregone problems, but for early intervention and prevention of disease in the whole child. In all children, actually. This same package of care can be used in service to population level public health needs where resources are a practical limitation, and yet there has been little focus on applying it that way. My dream is that one day it will be rural technicians and assistants presenting to academics at conferences on how they’ve adapted and improved these innovations to benefit their communities in the real world.
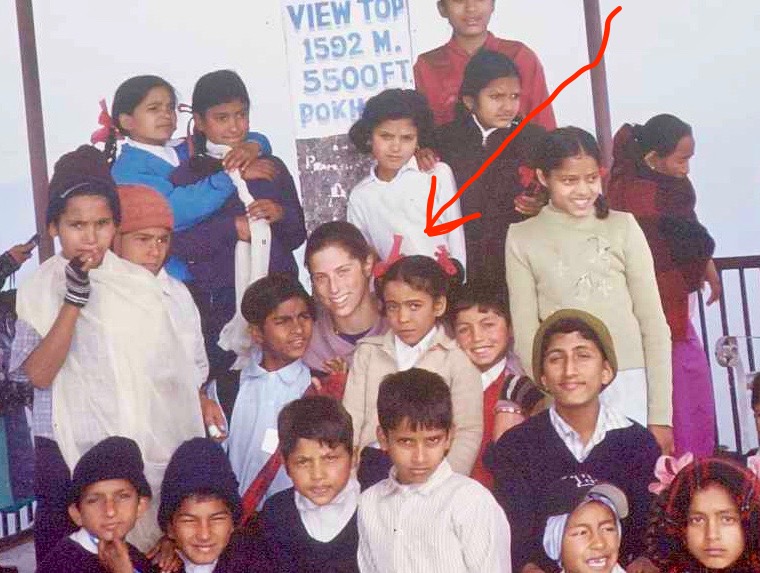
An incredible thing happened on the third day of our practice seminar in Kaskikot. The school we chose is next door to the Health Post. The third day was reserved for parents so that technicians could apply the training concepts to adult patients. I was waiting out in the stairwell when suddenly I saw a face I could never forget: Nisha, one of the students I taught for a year at Sada Shiva Primary when she was in fourth grade, a million years ago. It was with Nisha and her classmates that Govinda dai and I ran our first ever school oral health program back in 2004. At the end of that day, we took a photo of all of us in front of the Kaskikot Health Post, which at that time was just one simple building that today is fully dedicated to our Dental Clinic. Nisha had come to our seminar because her daughter is a student at the school where we were running the training in 2018–with five dental technicians, seven assistants, and an international expert in public health dentistry as trainer.

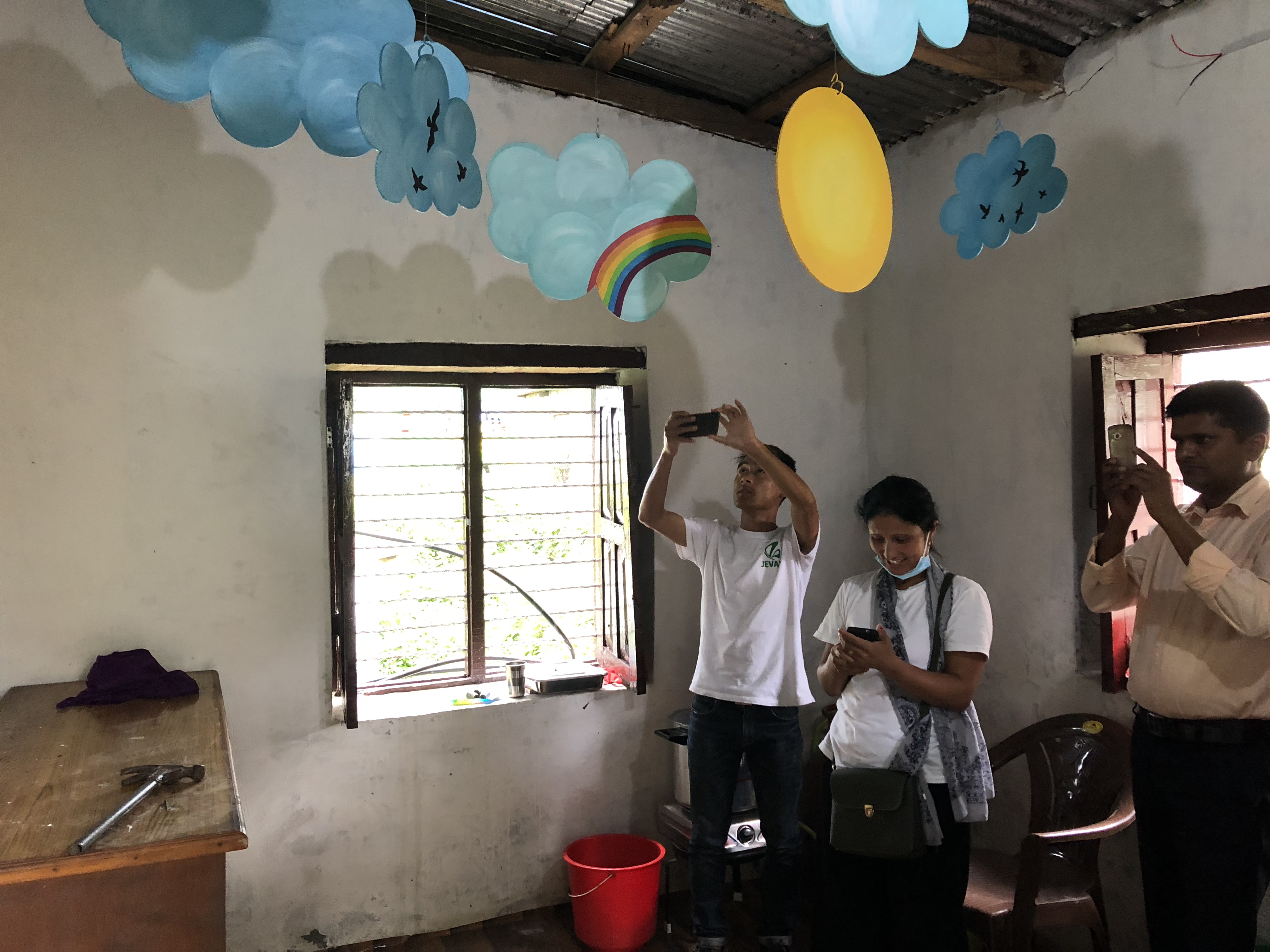
Finally, the icing on our professional development cake was a world-class makeover for the Kaskikot Clinic. My friend Maelle who lives in Pokhara started an organization called We Art One that paints murals and does art programs in schools. We asked We Art One to turn our Kaskikot Dental Clinic in to something bright and welcoming. They took it next level, putting this exuberant mural on the outside and literally building a ceiling mobile inside for patients to gaze at while lying in the chair. It’s made from hand-cut wooden clouds that Maelle painted.
I know not every rural Health Post in the world can have clouds and rainbows hanging from the ceiling. But I think they all should and I think we should try. The only reason we need is that every patient in the world is a person. Those of us with choices would never choose health care in an unfriendly, cold or unwelcoming environment, especially for medical treatment that can be scary like dentistry. I don’t know why we seem to believe in some kind of false economy that suggests it’s not realistic to afford that dignity to everyone. This beautiful artwork was not expensive or difficult; it was just a decision. It mattered more than doing something else for some other purpose.
So that was our summer. Two new clinics and nine veterans are open for business, if anyone out there needs an appointment! Come visit us soon!
2004:

2018: