These past few weeks, I increasingly find myself reliving the morning of April 25, 2015, when my phone woke me at 6:30am. I rolled over and Prem was on the line: a 7.8 magnitude earthquake had ripped through Nepal. I stumbled to the kitchen table in my slippers and didn’t move for what seemed like days. The papers were covered with images of fallen temples that were whole in my albums, with tent cities at familiar outdoor intersections in Kathmandu, with maps seen from high above and covered in digital markings. It was a long time before anyone could capture photos of people, especially in the rural expanses of the country, which were accessible only by helicopter for what seemed like ages. But in my mind’s eye the earthquake was a long, long parade of individuals. Today, I reread the email I sent out three days later.

It is a strange feeling to find the whole planet in crisis. Population-level disasters of this scale seem to disproportionately fall upon the shoulders and homes and rivers of the world’s most vulnerable places, while the other places try to help. In the years I have worked in Nepal, Nepali people have plodded on through civil war, three major government transitions, annual landslides and floods and hail, the 2015 earthquake, water shortages and electricity outages up to sixteen hours a day for years on end, and of course, the daily vulnerability of chronic poverty, weak infrastructure, and floppy safety regulations. The road to Kaskikot has had three bus accidents in the time I have considered it my second home. I remember thinking after the earthquake, as I watched messages flood my accounts, that people didn’t realize how often Nepal’s communities were used to seeing things broken, taken, lost, or never having existed in the first place. The earthquake was unthinkably horrible. Yet for those who didn’t lose everything–people, entire villages–that trauma was largely swallowed within a few months by massive shortages of petrol and goods due to political instability and border closings. The summer brought deadly landslides. Six months later, most of the country was no longer discussing the earthquake.
These last few weeks have been an odd, house-of-mirrors experience. While Nepal is facing pandemic, New York City and Milan and Barcelona and Sydney are also facing pandemic. My colleagues are quarantined in Pokhara and Kaskikot and Tilhar, and I’m quarantined in Hartford, and Prince Charles is quarantined in London. The realization that anything could happen to anyone at any moment has set upon us all, a realization that seems to be expanding daily. And amidst a great deal of chaos and uncertainty and worry, I find myself in occasional moments of disconcerting calm. Things were always this way. Now they are simply unveiled. We are all the defenseless Other.
 Now as then, there is great beauty to uncover in difficult times. In the months after the earthquake five years ago, we improvised. I have no idea how many kilometers Dilmaya and I walked. Practically speaking, I learned a huge amount about the contributions a small community-based organization like ours can offer in disaster management. At that time we found we were well placed to spend personalized time on unique household and community circumstances, to mitigate challenges that didn’t meet a universal disaster threshold but were extremely destabilizing for the specific individuals facing them. Our focus became “the lower percentage of damage:” the houses that were not fallen, but cracked and indeterminately unsafe. It was a life-changing experience.
Now as then, there is great beauty to uncover in difficult times. In the months after the earthquake five years ago, we improvised. I have no idea how many kilometers Dilmaya and I walked. Practically speaking, I learned a huge amount about the contributions a small community-based organization like ours can offer in disaster management. At that time we found we were well placed to spend personalized time on unique household and community circumstances, to mitigate challenges that didn’t meet a universal disaster threshold but were extremely destabilizing for the specific individuals facing them. Our focus became “the lower percentage of damage:” the houses that were not fallen, but cracked and indeterminately unsafe. It was a life-changing experience.
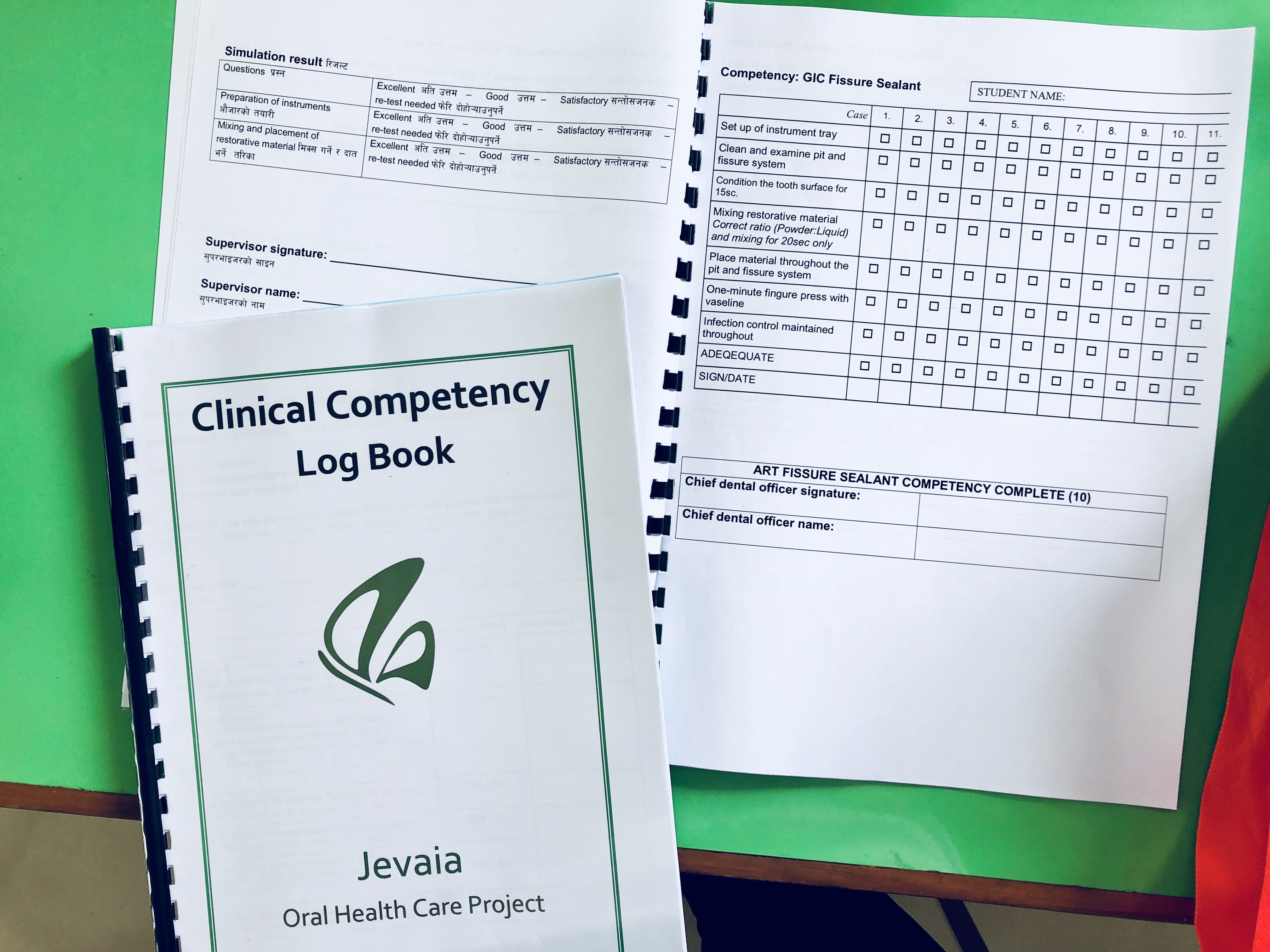
Every day this week I’ve joined in a group call with my colleagues in Nepal as they work from home, developing a strategy to redirect our rural health care personnel from dentistry to coronavirus. Since we launched our Dental Hub app in September, hundreds of patients and their phone numbers have been entered in our database, so our first step is having dental technicians replace their weekly clinics with “phone clinics,” calling every patient in the database. We’ve created a script for checking in with each family to see how well they’ve been able to implement isolation guidelines and what if any obstacles are in the way. We don’t yet know how this will go or how useful it will be, but it’s something to do. It’s a way to be in community.
All that said…the 2015 earthquake was irreconcilably different than the looming crisis we are facing now. To begin with, the rest of the planet is occupied with its own emergency, not fundraising and overloading the aid channels in Nepal with variably useful assistance strategies. Second, Nepal’s health care system was inadequate to meet public need before coronavirus, and there is effectively no intensive care available for severe Covid-19 cases. So even though there are so far very few confirmed coronavirus cases in Nepal, I am still trying to understand how “flattening the curve” works in a health care system where the capacity threshold is fairly close to zero. We don’t know the answer, if there is one. I’m not sure yet if anyone does.
Like many of us, I can’t help but wonder how we would understand our society if we felt this vulnerable and interdependent all the time. It is deeply unfamliar to us in the dominant American culture–replacing the community of work-productivity with the community of survival. Confronting the primacy of the nuclear family, when that family is cut off from neighbors, schools, social supports, food production, occupation, and future planning. This discomfort feels worthy of deep and shared reflection. In the mean time, I have made a call list, and have been doing one quality catch-up each day with someone I’ve missed, or who I want to make sure isn’t alone.
For whatever reason I also found myself drawn back this week to this poem, written during the (still unresolved) family separation crisis at the US border in the summer of 2018. I hope to use coming weeks to catch up on past entries and continue posting about the unfolding of this pandemic Nepal on my blog. In the mean time, wishing all of you patience and resilience and comfort as we, as a world, navigate the weeks and months ahead.
*
At the Base of a Tree
The cicadas came when I was five
behind the school yard.
I put my finger on one
and then I picked it up
it was like a fig, dark and rough.
At five cicadas were interesting, like figs.
Now I am much bigger
friendly, the little goat nuzzles my shoulder with his warm snout
soft, we are alive, together easily.
And then I press my eyes shut
as I capture the insect that has invaded this carpet, which is mine
because I own it.
Sometimes I wonder how I can find my way back
from the pliant kid to the figs to the cicadas, captivated
with all their legs, their slick ribbed shells, all their songs enchanting
the school yard
all chirping and chirping tickling my ears until my ears overflowed with music
amid the crunching leaves and delicate wings
a symphony, a society, a universe blossom
after seventeen years of silence.
Sometimes I wonder
what we are afraid of
why we crush things, bugs and leaves and oceans and people
when I was five, I used
just one tiny finger
to say hello.











































{kind=link}