The second half of our winter professional development is focused on treatment of older adults. Even though a lot of treatment that dental technicians do is in schools, during the weekly dental clinic at the Health Post, they mostly get adult patients. And since most rural adults have had little or no dental care, and likely weren’t exposed to fluoride toothpastes or other preventative measures for their first few decades of life, some of the conditions that present in our rural clinics are pretty extreme. Besides that, tooth loss in older age is common enough that it’s more or less expected.

Of course, our technicians can refer older patients to higher care, and they do. But following up on referrals isn’t always that easy, especially for older folks with reduced mobility. Not to mention that rehabilitation of many mouths we see in elderly patients would require months of ongoing, expensive, complex treatment even in a state-of-the-art dental hospital–something that’s simply is not feasible for the majority population even in a first-world city. So here we are in rural Nepal working in primary care, which is about disease prevention and improving quality of life. But save for the occasional extraction, older adults are mostly left out of the process when it comes to primary oral health care: directly related to the ability to eat, sleep, and participate socially. If we can relieve pain and preserve teeth longer, that seems like a solid contribution.
 With this in mind, we wanted to develop a professional development workshop on how the simple techniques that we’re already using – glass ionomer, silver diamine fluoride – can be used to help relieve the diseases experienced in older populations in Nepal. By “we” I mean Bethy since she’s the one obviously who did this because I write stories about teeth and she is a public health dentist. And even if you’re not a dentist or especially interested in cariology, I have to say that how this turned out is really pretty cool.
With this in mind, we wanted to develop a professional development workshop on how the simple techniques that we’re already using – glass ionomer, silver diamine fluoride – can be used to help relieve the diseases experienced in older populations in Nepal. By “we” I mean Bethy since she’s the one obviously who did this because I write stories about teeth and she is a public health dentist. And even if you’re not a dentist or especially interested in cariology, I have to say that how this turned out is really pretty cool.
A few years ago, Bethy and Keri took photos of about 65 people who’d had restorations done in our clinics, and we used these as the basis for a quality-of-care assessment. It resulted in a few different things. One was adding some missing instruments. Another was noticing an apparent pattern among older adults where, around middle adulthood, adult teeth begin to wear rather than decay. It might be caused by anything from an acidic diet, to abrasive brushing with spices, to a lifestyle change like a new medication. The lower part of the tooth near the gums wears down and become loose, causing sensitivity and difficulty eating, and gradually, the teeth simply fall out. These are the adults who, right now, are getting no care at all besides the occasional extraction. They were the focus of our training.
Our technicians practiced placing glass ionomer restorations on the root-surface lesions, near the gums, that so often lead to tooth loss in older adults. Bethy explained how an event in the life of a middle-aged adult, such as an illness, can cause a simple change like dry mouth that alters the whole environment and leads to deterioration of a previously resilient set of teeth over the next period of years.
I loved this workshop. For the first two hours, instead of looking at teeth, Bethy brought in pictures of older people and the clinical teams simply talked about aging. What makes people old? Are all old people the same? Do they have the same priorities and daily demands and ideas of self? What do we assume when we see someone who we think is “old”? How does a person’s identity factor in to how we work with them to improve their lives? What is our responsibility to someone’s dignity?
In preparing for the workshop, Bethy and I mined our respective photo archives for pictures of elderly people in Nepal and Cambodia. One by one their faces stared out at our group of clinicians, suddenly daring: Who do you think I am?
In the beginning, most participants had a sort of default position that older people are weaker and less capable of handling dental treatment. But as we went through the photos for well over an hour, stories blossomed. In some cases, they were people whose backgrounds we knew- my neighbors in Kaskikot, steely women I’d photographed during our work after the earthquake in 2015, caretakers and weavers and shopkeepers who’d given interviews in Bethy’s surveys in Cambodia. Bethy used a clever framework called “Go-go, go-slow, no-go” to talk about what each of these people might be expecting or hoping for from a medical professional.  I got to laugh about how Hadjur Aamaa has basically no teeth left and gets around pretty slow, but she’ll put one foot in front of the other to get to the house and then frets the entire day, every day, about the dishes or the peas that need to be shelled; it is absolutely vital to her human essence to be busy with something useful. By the end, our clinical teams were musing over what their patients might be thinking about, who they depended on, and who relied on them, what made them human and alive in the world. This was probably a go-slow patient, like Hadjur Aamaa; this one likely a go-go patient ready to sit there all day and get her teeth fixed; this patient probably wasn’t really about treatment, and mainly needed to have his discomfort acknowledged.
I got to laugh about how Hadjur Aamaa has basically no teeth left and gets around pretty slow, but she’ll put one foot in front of the other to get to the house and then frets the entire day, every day, about the dishes or the peas that need to be shelled; it is absolutely vital to her human essence to be busy with something useful. By the end, our clinical teams were musing over what their patients might be thinking about, who they depended on, and who relied on them, what made them human and alive in the world. This was probably a go-slow patient, like Hadjur Aamaa; this one likely a go-go patient ready to sit there all day and get her teeth fixed; this patient probably wasn’t really about treatment, and mainly needed to have his discomfort acknowledged.
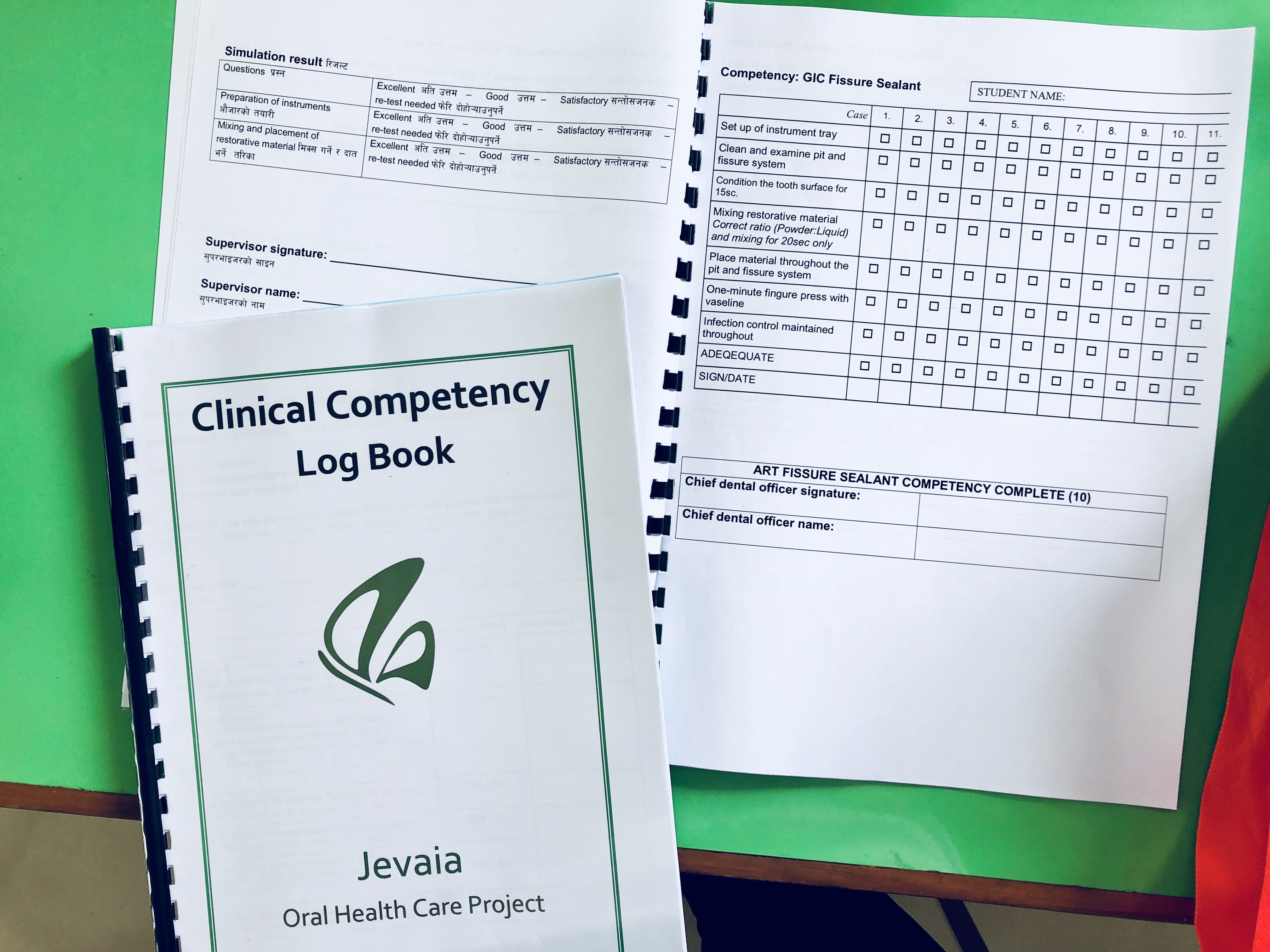
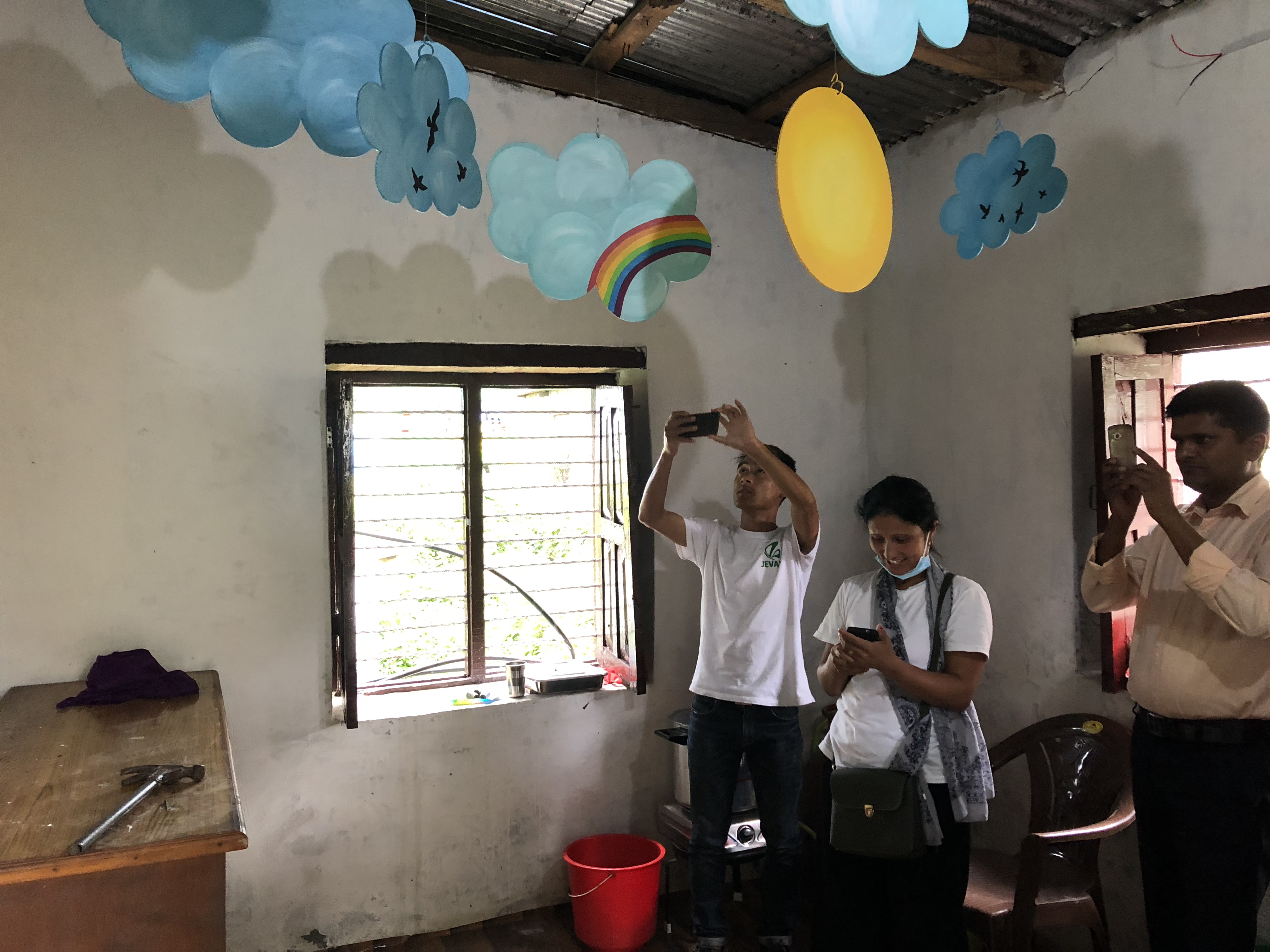
The next day, we returned to the same school in Kaskikot to treat patients age 45 and over. (We’re in rural Nepal, 45 is approaching the pre-elderly group…60 is safely considered “aged” and the point is to catch people BEFORE their teeth are gone.) It was exciting to see the same situations we’d learned about the previous day in the real lives of real people and to be able to offer simple treatments that have the potential to forestall tooth loss for years. The teams continued using the App, entering patient data digitally along side the paper forms.
While patients were waiting outside, the father in law of our local Channeler came by for a checkup. I’ve been to see our Channeler a few times – she lives down near Laushidunga, in the direction of Sada Shiva where I taught primary school for a year. The story that’s told about the Channeler is that she suffered terribly from a kind of delirium for a period of time. She was treated in a hospital, but nothing helped. Then she began to channel spirits. She rebalanced. People travel from all over to see her; I’ve brought a handful of visitors there to connect with people they’ve lost. Before Bishnu left for the U.S. in 2008, she went to see the Channeler to  connect with her father. The Channeler’s husband has a bum knee, and once I gave him my knee brace from CVS, and he always greets me with an old familiarity when we meet in the road up in Deurali.
connect with her father. The Channeler’s husband has a bum knee, and once I gave him my knee brace from CVS, and he always greets me with an old familiarity when we meet in the road up in Deurali.
Anyway, at some point in the afternoon I couldn’t find our technician K.P., and I walked outside to find he was having his palm read in the waiting area. The Channeler’s father in law spent about an hour reading almost everyone’s palm for fifty rupees each. Everyone–our office staff, the field teams, the schoolteachers and other patients–exclaimed over the things he knew: who’s father had died young, who was still to be married, who was destined to successfully stay with one line of work for a long time (one of our clinic assistants! yay!). I didn’t get a turn because by the time I was ready – I’d had my 50 rupees in my pocket for like an hour – he’d had enough with palm reading. Palm reading was over.
Still, my most favorite patient of the day was a 93 year old woman who arrived alone. She was  frail, used a walking stick, and barely spoke to anyone even to ask them to move out of the way as she plodded through clusters of people like Moses parting the sea. She wore a jaunty white knit cap that stuck up boisterously on her head. Her entire mouth was completely empty except for one jutting molar with an expanse of exposed root.
frail, used a walking stick, and barely spoke to anyone even to ask them to move out of the way as she plodded through clusters of people like Moses parting the sea. She wore a jaunty white knit cap that stuck up boisterously on her head. Her entire mouth was completely empty except for one jutting molar with an expanse of exposed root.
“How can we help you?” Hira, the Deurali technician, asked.
“This tooth hurts,” the woman said simply.
Hira treated the one tooth with silver diamine fluoride, a completely painless procedure that will hopefully preserve it a while longer and ease her suffering. Then the woman stood up, picked up her walking stick, parted the seas and went home without a word.
*